
Katherine Roberts
When the COVID-19 pandemic broke out in 2020, many conceptualised the challenge facing healthcare workers by describing it as a war. Nurses frequently adopted this martial analogy, describing themselves as soldiers serving on the frontline.i Some researchers argued that the best way for hospitals to respond to COVID was to adopt military protocol for mass casualty events, while others warned that healthcare workers would be likely to face levels of moral injury comparable to those experienced by soldiers.ii These analogies often drew on the experience of the Second World War as a multi-national reference point. Voices in the United Kingdom, the United States, and Canada drew on a popular belief in the bravery and camaraderie of their citizenry during the Second World War to boost morale, celebrate essential workers, and encourage adherence to lock-down regulations (See Figure 1).iii
Figure 1: Pop up message sent to nurses of the hospital system under consideration.iv
While these analogies were primarily rooted in the pandemic’s high mortality rate and the implementation of triage procedures, there is another wartime parallel that has not been fully considered: the need for nurses to assume the role of familial surrogate for their patients. Visitor restrictions implemented during the pandemic deprived patients of their family’s emotional support; nurses attempted to mitigate that loss by serving as patients’ primary support and the bridge between the patient and their absent loved ones. These restrictions recreated the circumstances that characterised military nurses’ provision of therapeutic care during the Second World War. Drawing on content analysis of survey data from nurses during COVID and close textual analysis of Second World War nurses’ personal documents, this paper considers the parallels between these two groups’ experiences of providing care for patients separated from their families. It argues that a comparison between these two data sets illustrates the impact of nursing’s increased professionalisation on the construction of therapeutic care while providing evidence of the consistent emotional need for this care from critical patient populations. This comparison demonstrates the importance of integrating historical study into nursing education to highlight these recurring patterns and illustrates how a historical perspective can be used to better prepare nurses to meet these challenges in the future.
Nursing and familial care
Popular understanding of familial care has been a key factor in establishing expectations for nursing since the emergence of Reform nursing in the mid-nineteenth century. In many ways, the family served as the model for the nurse. Professional nursing was intended to move the care of the ill and injured from the family home to the hospital while leaving the nature of that care unchanged. As historian Susan Reverby argues, nursing was initially ‘grounded in the expectation that caring was part of a woman’s duty to her family or community’ and, when that care shifted from unpaid labour provided by family to paid labour provided by strangers, the expectation remained that such labour ‘would still be a work of love’.v In her work to reform nursing and make it an acceptable profession for educated middle-class women, Florence Nightingale rooted the profession’s ideology within Victorian gendered assumptions regarding women’s innate caring abilities.vi This ideology transferred the sexual division of labour from the Victorian home into the Victorian hospital, casting the nurse, with her caring remit, in the role of mother, and patients in the role of her children.vii Nightingale’s strategy of using the image of the female nurse as mother to justify and de-stigmatise women’s presence within a hospital was also utilised by American women during the Civil War to secure their admission to military hospitals.viii
As Nightingale’s work in Crimea and Clara Barton’s efforts during the American Civil War demonstrate, this gendered understanding of therapeutic care was especially prevalent in female nurses’ efforts to gain access to military hospitals and was eventually adopted and promoted by American and British military leadership in the twentieth century. The military’s promulgation of this maternal image of the nurse served two key purposes. Firstly, as historian Ana Carden-Coyne argues, this focus on the ‘familial’ nature of military medicine, with doctors assuming the role of supportive father and nurses that of the caring mother/sister, assured the public that soldiers were receiving high quality care and, thereby, worked to mitigate the criticism that the military medical service was mechanistic and dehumanising.ix Secondly, the military, and the nurses themselves, highlighted the familial nature of nursing to allay anxiety over the potential for sexual impropriety in an environment where young unmarried women interacted closely with young men.x This familial construction of nursing was encapsulated by a First World War Red Cross propaganda poster, which depicted a nurse cradling a stretcher-bound soldier in her arms, above the words ‘The Greatest Mother in the World’ (See Figure 2).xi This construction remained prevalent in the United States, United Kingdom, and Canada throughout the Second World War and was still a powerful factor influencing American nurses’ understanding of their roles and responsibilities overseas during the Vietnam War.xii
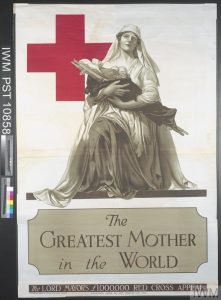
Figure 2: Alonzo Earl Foringer, The Greatest Mother in the World [poster] (London: Waterlow Bros & Layton Ltd., 1918): image courtesy of the Imperial War Museum
Beyond the protection that this construction offered from scandal and suspicion, nurses highlighted the comfort that their patients appeared to derive from their assumption of a familial role. In her discussion of First World War nursing, historian Christine Hallett draws on Wilfred Bion’s theory of containment to argue that nurses adopted a maternal position to provide their patients with the psychological support necessary to process traumatic wartime experiences.xiii This affiliation of a maternal figure with psychological and emotional support is long-standing. In a 1939 article published in the Nursing Mirror, psychiatrist Charles Stanford Read argued that ‘It is largely the child within us that makes us afraid. To her terrified patient the nurse assumes the role of a mother’.xiv By assuming this maternal position, nurses provided their patients with a ‘safe’ and ‘familiar’ space to process their injuries and allowed them to do so before having to confront their families. Both Carol Acton and Christine Hallett argue that, by serving as proxy mothers/sisters, nurses protected patients’ families from the worst of what their loved ones had suffered and reassured their patients of a positive reception from their families following their convalescence.xv
The adoption of a familial role also offered nurses a way to offer therapeutic care in a structured and bounded manner, which protected both nurses and their patients from inappropriate emotional entanglements.xvi While this construction of therapeutic care offered nurses a familiar scaffolding on which to build their practice, it was one plagued with potential pitfalls. This construction of nurse-as-mother was highly idealised and emphasised nurturing and self-abnegation over all else, even the nurse’s own well-being.xviiNurses were expected to embody not only ‘mother’ but ‘The Greatest Mother in the World’.xviii With its connection to the nurse’s gender, this construction also presumed that all female nurses had the innate ability to offer the necessary level of therapeutic care to profoundly ill or injured patients, a skill that is neither innate nor easy to acquire.xix However, should a nurse be unable to meet these expectations of kindly, maternal care, she could be perceived as a failure and met with antipathy and resentment from her patients.xx Additionally, by connecting therapeutic care to an innate gendered ability, this construction dismissed and denigrated the skill that it took to deliver it.xxi
In many ways, it was this gendered connection between the female nurse and ‘motherly’ care that nursing sought to distance itself from throughout its increasing professionalisation during the twentieth century. As Roberta Bivins, Stephanie Tierney, and Kate Seers argue, this process and the accompanying ‘changes in educational models and pathways to professional advancement have largely … rewarded nurses for specialisation and management roles, while “skilled bedside nursing”’, care that had previously been constructed as motherly, did not receive similar levels of attention and support.xxii However, this kind of therapeutic nursing has found advocates in palliative and compassionate care, and, while the literature within these fields has worked to avoid returning to the nurse-as-mother narrative, the notion of family-like care has remained influential.
Nursing theorists in this field argue that a patient in hospital experiences a particular vulnerability that creates a moral obligation for the nurse to care for them.xxiii That patient’s vulnerability is derived from two key sources. Firstly, they are wrestling with the dis-regulating and threatening experience of serious injury or illness, which disrupts an individual’s sense of safety and comfort within their body.xxiv Secondly, this physical vulnerability is exacerbated by the fact that it requires that the patient allow a nurse to care for their body, instead of restricting that intimate interaction to a known and trusted individual, such as a family member.xxv
Within compassionate care practice, the nurse works to address the second component of a patient’s vulnerability by creating a trusting intersubjective relationship through her therapeutic use of self. There are three key factors that establish a trusting relationship between patient and nurse: firstly, the patient feels safe, both emotionally and physically, with their nurse; secondly, the patient feels that the nurse acknowledges them as a unique individual; and thirdly, the patient knows that their suffering is seen and recognised by the nurse.xxvi The establishment of this trusting relationship does not eliminate vulnerability but rather establishes a degree of reciprocal vulnerability, closer to that experienced in relationships with family and friends. While the patient’s vulnerability remains pre-eminent, both nurse and patient experience being placed into a situation of great intimacy and intensity with someone who is a stranger to them.xxvii
Within compassionate care literature, the familial bond is a common point of reference and authors will utilise terms like ‘companionship’, ‘kinship’, and ‘love’ to describe the nurse-patient relationship.xxviii Prior to the pandemic, palliative care appeared to be the primary area acknowledging nurses taking on a familial role, with research discussing how hospice nurses drew on their understanding of familial bonds to structure their care and their grief at their patients’ deaths.xxix A key exception to this trend lies in the research surrounding the experiences of modern military nurses on deployment. In their analysis of interviews with nurses from the Australian Defence Forces, Andrew Ormsby, Ann Harrington, and Sally Borbasi found that ‘participants perceived that they had an important role in the provision of spiritual care in the absence of family on deployed operations’ and that these nurses ‘often adopted the roles of siblings and parents to personnel when deployed’.xxx
During the pandemic, visitor restrictions produced circumstances that mirrored those experienced by deployed military nurses and highlighted the nurse’s role as a familial surrogate. This is reflected in the literature that has been produced since 2020, with more research addressing nurses acting as family. However, the majority of this research has discussed this role within the context of pandemic palliative care.xxxi This paper argues that consideration of the nurse-as-family-surrogate needs to be expanded beyond palliative care to sufficiently prepare nurses for confronting the circumstances that a pandemic like COVID-19 creates. The parallels present between Second World War and pandemic nursing experiences demonstrate that this demand for familial care, however it might be expressed, is a consistent one when a patient population is separated from their traditional support network.
Sources and methodology
This paper is rooted in a comparison between the analysis of two data sets. The first is an anonymous survey of nurses working during the COVID-19 pandemic at a mid-Atlantic hospital system in the United States. The survey contains responses from 195 participants and was examined using content analysis, which highlights common themes present throughout the data.xxxii This analysis was undertaken by the author and two other researchers, who settled on the key themes present in the data through joint analysis and collaboration.xxxiii The second data set consists of personal documents written by seven Queen Alexandra’s Imperial Military Nursing Service Sisters (QAs) over the course of the Second World War, including four diaries and three collections of letters.xxxiv These documents were examined by the author using close textual analysis, which takes into consideration the documents’ physical and literary content.xxxv
While these data sets are disparate in many ways – from the type of data under consideration, to the means of analysis, to the temporal and cultural context in which the data was produced – the theme of the nurse serving as a familial surrogate was notably present in both. Nurses during COVID emphasised the impact of visitor restrictions and subsequent family absence on their patients and their provision of care. Similarly, Second World War QAs ruminated on the impact that the expectation that they would consistently serve as emotional support for their soldier-patients had on their practice. This paper examines how this theme was presented in these two different contexts and considers what lessons can be learned from its continuity over time.
Results
Nurses within both data sets acknowledged acting in a familial manner towards their patients and serving as their family surrogates. Nurses working during COVID explicitly addressed this element of their practice, with one survey respondent writing that ‘the nurses have become the stand ins for family’.xxxvi Another seconded this opinion, writing that ‘nurses stood in as surrogate family members’.xxxvii A third reiterated that ‘We have become more like their family than ever before’.xxxviii Notably, these nurses described themselves as acting in a generalised family-like manner and did not adopt any specific family role. In contrast to this, the cultural context of early twentieth century nursing expected that QAs would perform the role of mother/sister to their patients. In their personal documents, QAs did not often explicitly state that they were acting as family. Sister Agnes Morgan’s statement in a January 1942 letter that ‘I do my best and try to be most motherly’ serves as the exception rather than the rule.xxxix However, the QAs’ adoption of a maternal/sororal role was evident in the language they used to describe their patients, often taking on a parental affectionate tone. It was common for nurses to refer to patients as their ‘boys’, casting them as children.xl In her letter recounting her efforts to be ‘motherly’, Sister Morgan described helping an injured patient participate in a Christmas sing-along, calling him ‘my own little, very, very ill boy’.xli In a November 1942 diary entry recording the loss of one of her patients to malaria, Sister Nell Jarrett sadly wrote that ‘My boy has died’.xlii
Overall, there were three common characteristics present in these nurses’ performance of a family surrogate role. These characteristics align with the recommendations from compassionate care literature on the elements necessary to form a trusting intersubjective relationship. They include the nurse’s use of their physical presence to provide company, comfort, and mitigate fear; an increase in reciprocal intimacy between nurse and patient; and the nurse serving as a bridge between the patient and their absent family, which often required the nurse to become intimately involved in communication between loved ones. However, the manner in which these common characteristics were expressed remained tied to the cultural context within which the nurses found themselves, with QAs taking on the maternal persona that the gendered understanding of their profession encouraged and COVID nurses adopting a more amorphous familial role.
The use of presence
Research addressing COVID-19 visitor restrictions has highlighted the importance of family presence to patient well-being and the negative impact resulting from its removal. In their review of current research, Karin Hugelius, Nahoko Harada, and Miki Marutani emphasise that the social support patients receive from family and close friends is critical in mitigating patient distress and that, amongst critical care patients, the presence of family ‘is often a strong motivation to stay alive and to continue the struggle to recover’.xliii The removal of this support has proven to have serious consequences, resulting in increased incidences of depression, anxiety, aggression, and pain amongst patients.xliv One COVID nurse noted that visitor restrictions highlighted ‘the hunger patients had for human contact when they were in isolation. Often it was the nurse that was the only consistent human contact’.xlv Another commented that, without the support of their families, many patients were ‘turning to a very depressed and hopeless place’.xlvi While Second World War military patients were not subject to visitor restrictions like those experienced during COVID, their loved ones remained just as far removed. In a diary entry written while working on a psychiatric ward, Sister Mary Morris credited her patients’ psychiatric injuries to a combination of battlefield trauma and their ‘enforced separation from their families’.xlvii
Both COVID nurses and QAs were confronted with lonely, frightened patient populations and sought to mitigate their distress by taking on a family role, standing in for the people their patients were missing. These nurses worked to mitigate the lack of familial support through such things as comforting touch, active listening, and ‘presencing’, or ‘being present and available to the patient’.xlviii These actions aimed to create a safe and supportive space for patients in the absence of their traditional support system. One COVID respondent noted that many patients ‘are upset and feel lonely’ and, therefore, the nursing staff ‘have to be there to help them emotionally’.xlix Another respondent connected this emotional help to their physical presence, writing ‘I find that I am spending more time in the rooms assisting patients and talking to them to be their emotional support’.l A third respondent highlighted how emotional patients would become after speaking with their family via FaceTime, explaining that eventually ‘I’ve been unable to just walk out. I just couldn’t do it … I would sit in a chair 6 feet away and talk’.li In response to the distress that patients experienced from the loss of the comfort of their family’s physical presence, nurses offered up their own presence to meet their patients’ need.
COVID nurses emphasised the importance of the nurse’s presence in palliative care situations. One respondent recounted being assigned a single COVID patient, ‘who was actively dying. My job that night was to be in close contact with the patient’s family member and to just sit and hold her hand so that she didn’t die alone’, taking on a role that previously would have been held by that patient’s family.lii Another respondent highlighted the importance of the nurse’s presence in these moments, writing that ‘I try to go into the dying patients’ rooms more frequently and I try to run in there if death is imminent so they are not alone’ before admitting that this demand for presence ‘puts a heavy emotional burden on us nurses that was previously on the family’, directly acknowledging the nurse’s assumption of the family’s role.liii This connection between presence and a familial role was also present in communications from the hospital’s leadership team in the midst of the first wave of COVID. In a hospital newsletter, the Chief Nursing Officer praised the nursing team for ‘being the family for the patient since we cannot allow visitors’ and thanked staff for the care they had offered patients who had died, highlighting the nurses’ presence ‘at their side, holding their hand, being their family’.liv
Similar uses of the nurse’s presence as a source of comfort can be found throughout the writings of Second World War QAs. In a February 1943 letter, Sister Agnes Morgan wrote to her mother:
I have a very, very ill boy called ‘Tommy’ … and at present he is going through a stage of ‘wandering’ in which he gets very frightened, so I spend a good part of every night with him, and tonight it was quite impossible to leave him at all before he dropped off to sleep; so there I was … clutched by the hot hands of my poor friend.lv
Clearly, Morgan’s physical presence and use of therapeutic touch were critical to her perception of providing comfort and a sense of safety to her patient. Similarly, in a December 1940 diary entry, Sister Joyce Ffoulkes-Parry described offering her presence as a comfort to a patient, who had just learned that his parents had been killed in an air raid in the United Kingdom:
Poor Morris, no one had been near him all day – I suppose they would feel that he wanted to get away – but he did want to talk about it and go over and over it. I felt that he did so I went to sit on his bed … and stayed with him for a very long time.lvi
Sister Mary Morris’ use of therapeutic touch and her physical presence to bring comfort to distressed patients can be seen in her interactions with Lieutenant Martin, a shell-shocked officer, whose traumatic experiences had rendered him mute. In a 28 June 1944 entry, Morris wrote that ‘Lt. Martin seems to be a little less withdrawn … He smiled at me as I held his hand and talked to him’.lvii
The influence of the different cultural contexts in which this care was delivered can be seen in the manner in which these two populations of nurses discussed this use of their physical presence. While COVID nurses explained that they were intentionally using their physical presence to provide their patients with emotional support as a part of their nursing care, QAs did not present these moments as expressions of professional practice but rather as the actions of a caring woman, structuring their provision of therapeutic care within the cultural perception of the nurse as mother. In spite of the different ways in which these two cohorts of nurses talked about the care they offered, the care itself often looked the same, with the nurse being present, engaged, and, occasionally, in physical contact with a vulnerable person in distress. This provided patients with the emotional comfort and support that, under different circumstances, would have been provided by their family.
Increase of reciprocal intimacy
One of the key elements in the establishment of a trusting intersubjective relationship between nurse and patient is the patient’s sense that their nurse ‘knows’ them.lviii In pursuit of this trusting relationship, some researchers have encouraged nurses to engage in biographical work with patients and their families to strengthen the nurse-patient relationship, advocating for nurses to come to know their patients as individuals.lix This need on the part of the patient to be ‘known’ to their nurse is not a recent development. Professor Carden-Coyne argues that a key complaint put forward by military patients during the First World War was that military medicine was mechanistic and depersonalised.lx These patients did not feel that they were known by the people who cared for them, and this negatively impacted their experience of that care. Similarly, Professor Christine Hallett contends that many First World War nurses saw that a key element of their role was to help their patients reconnect with their humanity and individuality after the degrading experience of trench warfare.lxi These women worked to help their patients come to know themselves again, developing familiarity and intimacy with them along the way. This need for nurses to help patients regain their sense of self following the dehumanising experience of both military training and combat continued through the Second World War as well.
Nurses during both the Second World War and the COVID pandemic recognised the importance of demonstrating a willingness to ‘know’ their patients to that patient’s well-being and sought to integrate that into their provision of care. One COVID respondent noted that they experienced more ‘connectedness with patients in the absence of visitors’.lxii Another found that patients were ‘more receptive to emotional engagement because … they are more isolated’, while a third stated ‘I honestly feel like I’ve been able to connect with my patients on a more personal level since the pandemic, as we are some of the only people they will see during their entire hospital stay’.lxiii Deprived of their usual sources of emotional support, isolated patients opened up and attempted to make themselves known to their nurses and their nurses made themselves available for these disclosures. Nurses further facilitated the development of a sense of ‘knowing’ one another by occasionally reciprocating these disclosures. A COVID respondent addressed this relational reciprocity, writing that ‘my patients will ask more personal questions about how the pandemic has impacted me both personally and professionally’.lxiv This reciprocal connection worked to increase patient comfort and a sense of safety with their nurse, as this increased level of mutual disclosure changed the nurse from a stranger to someone who more closely resembled family.lxv
COVID nurses approached this increased intimacy between themselves and their patients in an individualised manner, adapting to each unique patient. As such, their familial care was not structured by a set gendered expectation. Overall, their discussions of this care reflected the multi-gender, multi-generational nature of both the nursing and patient populations, with respondents commenting that they attempted to treat patients like they were ‘my mother or father’ or ‘my mom or son’.lxvi In contrast to this, the gendered construction of nursing during the Second World War pushed QAs to structure this increased intimacy with their patients within the framework of the nurse-as-mother, an approach that appeared to be expected and accepted by their patients. The all-female QAs came to ‘know’ their patients through the role of temporary mother/sister, while their male patients made themselves ‘known’ to their nurse through the role of temporary child/brother.
Sister Morgan’s comment regarding her efforts to be ‘most motherly’ occurred within the context of her first Christmas abroad where she wrote that ’40 out of 50 “soldiers” present thought of their mothers while they sang! We seem so far away from them and so lonely, and Christmas isn’t right without Mums somewhere near!’.lxvii Morgan offered supportive care to her patients by stepping into the role of their absent mothers to give their holiday celebrations a sense of ‘home’. Patients aided the QAs in their attempts to recreate ‘home’ by sharing the details of their home life with them. In her Christmas letter, Morgan wrote that ‘This is the kind of day when everybody shows me their photographs of home’.lxviii This kind of intimacy was not limited to the holidays. In an October 1944 diary entry, Sister Morris noted that an American patient ‘has invited me to visit his home in Texas after the war and shown me photographs of Mom and Pop and his kid sister. I receive many invitations such as this’.lxix This sharing of personal information was not limited to the patients but was reciprocated by the nurses themselves. In a February 1943 letter, Sister Morgan described caring for a soldier who had lost a leg ‘and hadn’t yet recovered from the shock … We became great friends over night, part of which I spent knitting by his bed; with the result that by the morning he knew all about my niece, and who my knitting was for!’.lxx Morgan later described this patient asking for updates on her niece and to see her picture.
Wartime QAs were quick to highlight any point of commonality that they shared with their patients and a key one that they relied on was their position as women from their patients’ home country and, therefore, as an embodied connection to their home lives and families. In a letter to her parents, Sister Vera Jones described treating a patient from her home county of Essex, writing that they ‘often discuss Essex, and when I see him I greet him with, “Hello Chelmsford”, and he says “Hello Maldon”’, explaining that patients ‘love to meet someone who knows their own county’.lxxi Sister Ffoulkes-Parry noted a similar desire for connection from her Australian patients, who were consistently happy to learn that she was an Australian herself, observing that ‘they seem pleased to know that there was someone more or less belonging to them’.lxxii In an October 1943 letter, Morgan, a Liverpool native, described how she encouraged her patient, a fellow Liverpudlian, through the acute stages of diphtheria ‘with thoughts of the hometown’ they shared.lxxiii
As these examples indicate, the establishment of an increasingly intimate nurse-patient relationship was a reciprocal process, wherein the nurse became known to the patient just as the patient became known to the nurse. This reciprocal connection worked to increase patient comfort and a sense of safety with their nurse.lxxiv However, this increased intimacy also presented increased emotional risk to the nurses as the development of a more family-like relationship potentially exposed the nurse to more intense grief should the patient die.
The nurse as a bridge
A key role that nurses adopted during the COVID-19 pandemic and the Second World War was serving as a bridge between patients and their absent family. This often required that nurses become intimately involved in the communication between loved ones, making the nurse a witness to, and participant in, situations that previously would have been entirely private.
During the Second World War, QAs served as the means of communication between patients and their families, as they were often responsible for taking dictation from patients or composing letters on their behalf. In a September 1944 letter, Sister Vera Jones explained that ‘I receive all sorts of messages from the relatives to give to the men, and the patients send messages back through me’.lxxv In a November 1944 letter, she elaborated on her integration into her patients’ lives and families:
I have a very large mail from relatives of seriously ill patients … They write to me like old friends inviting me to go and see them when I go home. The patients are always so grateful to me for writing. When I go round the wards one of them often says to me, ‘Have you heard from my mother lately? She has written to me and asks me to give you her love’.lxxvi
Jones’ involvement in her patients’ communications with their families was not unusual. In a 1940 diary entry describing her work with a patient with tetanus and pneumonia, Sister Helen Luker recorded that she came on duty to find her patient ‘rather miserable … I wrote letters for him and tried to cheer him up generally’.lxxviiIn a later entry, she noted that ‘Jones is still improving … and I have had a letter from his wife’.lxxviii In a 1941 letter, Sister Morgan wrote that one of her young patients ‘knows that he is very ill, but we’ve made all sorts of plans for “after the war”, and we compose air graphs to his mother between us’.lxxix
With the implementation of visitor restrictions, nurses working during COVID found themselves responsible for facilitating contact and communication between patients and their families. One respondent explained that nurses ‘interacted heavily with patient’s families … and really became their sole source of knowledge and support about their loved ones’.lxxx Another stated that nurses were ‘the only life line that the patients family has to them’, while a third mused that visitor restrictions had made them ‘close to their [the patients’] problems’ in a way that they hadn’t been previously.lxxxi Respondents described facilitating patients’ access to technology to communicate with their family, at times using their own personal cell phones.lxxxii
Serving as a bridge between the patient and their family became especially important when nurses were providing palliative care. During the Second World War, while the War Office provided families with notifications of their loved one’s death, it was often the patient’s nurse who gave his family a full account of his death. Sister Vera Jones admitted that the ‘hardest thing is writing to tell of the person’s death, because I feel that the airgraph will be treasured ever afterwards so I put my best into it. I often have such grateful replies’.lxxxiii In a November 1944 letter, Jones described the close connection and continued involvement with a patient’s family that this role produced, writing that ‘One poor woman whose son died here, still writes. Matron and I went to the cemetery recently and took a photo of his grave. We hope it will turn out well, as we want it to send to her’.lxxxiv
Much like the QAs, nurses working during COVID-19 often found themselves responsible for bearing witness to a patient’s last moments and conveying those moments to their family. One respondent noted that as ‘most families were not allowed at the bedside, [nurses] had to be there for the patients at time of death’.lxxxvAnother respondent commented on the role that nurses played in facilitating the virtual presence of family members, writing that ‘Facetiming the patients’ families has been a big change because of the pandemic. It can be very sad to stand there and hold the … phone intron[sic] of their very sick loved ones and hearing what they say to them’.lxxxvi With the use of technology such as FaceTime, nurses became the family’s avatar, enabling them to see and speak to their dying loved one, while providing the physical comfort that the family was incapable of delivering, such as being physically present and holding the patient’s hand.
Without modern communication technology, QAs were required to take this embodiment of the patient’s family even further. While modern nurses could fulfil the family’s physical role while using cell phones to allow the family to see and speak to the patient, QAs had to fully take on the role of family at a patient’s death, providing both physical and verbal comfort. This need to have the nurse embody the family at the time of death exposed nurses to a level of emotional intensity with patients and their families that they would not have experienced previously. As Sister Iris Hooper explained in a June 1945 letter published in the Medical Gazette, ‘the greatest emotional strain was caused by being audience to the domestic and personal side of a life fast ebbing from one who seemed to have so much to live for’.lxxxvii Echoing this sentiment, one COVID respondent commented that ‘I felt that I carried more emotional responsibility with each patient in isolation’.lxxxviii Another addressed the burden placed on nurses by the need to serve as the family’s avatar, explaining that ‘facetiming with the patients and their families have been some of the most difficult moments emotionally’.lxxxix Serving as a familial surrogate in this manner was difficult and distressing for nursing staff yet they believed that it was an important role and one that needed to be performed in order to successfully care for their patients.
Conclusion
Both Second World War QAs and nurses working during the COVID-19 pandemic took on the role of familial surrogate in response to the emotional needs of their isolated patient populations. While patients’ need for familial support remained consistent, the differing cultural contexts in which these two nursing populations worked impacted the delivery of this family-like care.
The gendered construction of nursing during the Second World War provided structure to nurses’ provision of familial therapeutic care. QAs knew what kind of familial role they were supposed to play: that of the mother/sister. While this construction informed their care delivery, it also proved to be problematic. The nurse-as-mother construction was both highly idealised, demanding perfection in its execution, and viewed as an innate ability possessed by all women, diminishing the experience and effort necessary to deliver therapeutic care.
Given modern nursing’s shift away from such gendered constructions, nurses working during COVID-19 found their provision of familial care lacking these structured gendered expectations and instead adopted a more generalised family-like role. Modern literature addressing compassionate care has emphasised the difficulty and skill necessary to provide this kind of therapeutic care and its importance to patient well-being; however, much of the discussion of nurses serving in a familial role has remained siloed within palliative care research.
The parallels between the experiences of Second World War QAs and COVID-19 nurses demonstrate the potential pitfalls of keeping familial care isolated in one speciality. Patients’ need for familial support is not a momentary aberration but rather a consistent element that nurses must prepare for, especially when they are confronted with circumstances in which the patient’s normal sources of support are absent. A more thorough integration of nursing history into nursing education has the benefit of highlighting these parallels, providing the profession the opportunity to proactively identify and prepare for such needs before another crisis brings them to the fore.
Endnotes
i Ilkay Dagyaran, Signe Stelling Risom, Selina Kikkenborg Berg, Ida Elisabeth Højskov, Malin Heiden, Camilla Bernild, Signe Westh Christensen, and Malene Missel. ‘Like Soldiers on the Front – a Qualitative Study Understanding the Frontline Healthcare Professionals’ Experience of Treating and Caring for Patients with COVID-19.’ BMC Health Services Research 21/1 (2021), 5; Paula Manuela Jorge Diogo, Maria Odete Carvalho Lemos e Sousa, Joana Rita Guarda da Venda Rodrigues, Tânia Alexandra de Almeida Martins de Almeida e Silva, and Márcia Leandra Ferreira Santos, ‘Emotional Labor of Nurses in the Front Line against the COVID-19 Pandemic’, Revista Brasileira de Enfermagem 74 (2021), 4.
ii Robert Anders, ‘What Can We Learn from U.S. Military Nursing and COVID-19?’ Nursing Inquiry 27/4 (2020); Neil Greenberg, Mary Docherty, Sam Gnanapragasam, and Simon Wessely. ‘Managing Mental Health Challenges Faced by Healthcare Workers during Covid-19 Pandemic’, BMJ 368 (2020), 4.
iii James Hill, Artist Finds Inspiration in War Propaganda for COVID-19 “Stay In” Posters, ABC News, (2020). Available at: https://abcnews.go.com/US/artist-finds-inspiration-war-propagandacovid-19-stay/story?id=70732034 [Accessed 13 July 2023]; Martin Maxwell, Martin Maxwell on COVID-19: This Generation’s Great War, National Post, (2020). Available at: https://nationalpost.com/opinion/martin-maxwell-on-covid-19-this-generationsgreat-War [Accessed 13 July 2023]; David Hunter, Coronavirus: If We Are in a War against COVID-19 Then We Need to Know Where the Enemy Is, The Conversation, (2020). Available at:http://theconversation.com/coronavirusif-we-are-in-a-war-against-covid-19-then-we-need-to-know-where-the-enemy-is-135274 [Accessed 13 July 2023]; Helena Vesty, The Incredible Story of Sacrifice by Salford Royal Nurses Nearly 80 Years Ago, Manchester Evening News, (2020). Available at:https://www.manchestereveningnews.co.uk/news/greater-manchester-news/incredible-storybravery-sacrifice-nurses-18455221 [Accessed 13 July 2023].
iv Image courtesy of Joanna Dixon, Main Line Health Center
v Susan Reverby, Ordered to Care: The Dilemma of American Nursing, 1850-1945. (Cambridge: University Press, 1987), 2.
vi Maggie Boulton, Anna Garnett, and Fiona Webster, ‘A Foucauldian Discourse Analysis of Media Reporting on the Nurse-as-Hero during COVID-19’, Nursing Inquiry 29/3 (2022), 3-4.
vii Deborah Palmer, ‘“To Help a Million Sick, You Must Kill a Few Nurses”: Nurses’ Occupational Health, 1890–1914’, Nursing History Review 20/1 (2012), 24; Reverby, Ordered to Care, 24-25, 41-42; Kara Dixon Vuic, ‘Wartime Nursing and Power’, in Routledge Handbook on the Global History of Nursing, ed. by Patricia D’Antonio, Julie Fairman, and Jean Whelan. (Abingdon, Oxon: Routledge/Taylor & Francis Group), 2013, 23.
viii Vuic, ‘Wartime Nursing and Power’, 23-24.
ix Ana Carden-Coyne, The Politics of Wounds: Military Patients and Medical Power in the First World War(Oxford: Oxford University Press, 2014), 191-192.
x Jane Brooks, Negotiating Nursing: British Army Sisters and Soldiers in the Second World War(Manchester: Manchester University Press, 2018), 25, 29; Carden-Coyne, The Politics of Wounds, 196.
xi Alonzo Earl Foringer, The Greatest Mother in the World 1918 [poster] (London: Waterlow Bros & Layton Ltd., 1918): copy held by Imperial War Museum, Art.IWM PST 10858.
xii Carol Acton, ‘Bodies Do Count: American Nurses Mourn the Catastrophe of Vietnam’, in The Memory of Catastrophe, ed. by Peter Gray and Kendrick Oliver. (Manchester: Manchester University Press, 2004), 159, 165; Kara Dixon Vuic, Officer, Nurse, Woman: The Army Nurse Corps in the Vietnam War (Baltimore: Johns Hopkins University Press, 2010), 150, 154, 189.
xiii Christine Hallett, Containing Trauma: Nursing Work in the First World War (Manchester: Manchester University Press, 2010), 165.
xiv Charles Stanford Read, ‘The Nursing and the Psychological Emergencies of War’, The Nursing Mirror, 16 September 1939, 319, as quoted in Jane Brooks, ‘“Not Only with Thy Hands, But Also with Thy Minds”: Salvaging Psychologically Damaged Soldiers in the Second World War’, Nursing History Review 27 (2019), 40.
xv Carol Acton, ‘Negotiating Injury and Masculinity in the First World War Nurses’ Writing’, in First World War Nursing: New Perspectives, ed. by Alison Fell and Christine Hallett, (New York: Routledge, 2013), 126; Christine Hallett, ‘Emotional Containment: Nurses and Resilience.’ In The First World War and Health: Rethinking Resilience, ed. by Leo van Bergen and Eric Vermetten. (Leiden; Brill, 2020), 250.
xvi Acton, ‘Negotiating Injury’, 128; Hallett, Containing Trauma, 177, 178.
xvii Carol Acton and Jane Potter, Working in a World of Hurt: Trauma and Resilience in the Narratives of Medical Personnel in Warzones. (Manchester: Manchester University Press, 2015), 37.
xviii Foringer, The Greatest Mother in the World.
xix Hallett, ‘Emotional Containment’, 250.
xx Carden-Coyne, The Politics of Wounds, 198, 244.
xxi Hallett, Containing Trauma, 175.
xxii Roberta Bivins, Stephanie Tierney, and Kate Seers, ‘Compassionate Care: Not Easy, Not Free, Not Only Nurses’ BMJ Quality & Safety 26/12 (2017), 1024.
xxiii Marit Helene Hem and Kristin Heggen, ‘Is Compassion Essential to Nursing Practice?’, Contemporary Nurse 17/1–2 (2004), 19; Pam Smith, The Emotional Labour of Nursing Revisited: Can Nurses Still Care? (Basingstoke: Palgrave Macmillan, 2012), 2-3.
xxiv Jan Draper, ‘Embodied Practice: Rediscovering the “Heart” of Nursing’, Journal of Advanced Nursing70/10 (2014), 2237; Sanne Angel and Solfrid Vatne. ‘Vulnerability in Patients and Nurses and the Mutual Vulnerability in the Patient–Nurse Relationship’, Journal of Clinical Nursing 26/9–10 (2017), 1433.
xxv Deborah Lupton, ‘“Your Life in Their Hands”: Trust in the Medical Encounter’, in Health and the Sociology of Emotions, ed. by Veronica James and Jonathan Gabe (Oxford: Blackwell Publishers, 1996), 168; Miriam Moss, Sidney Moss, Robert Rubinstein, and Helen Black, ‘The Metaphor of “Family” in Staff Communication About Dying and Death’, The Journals of Gerontology: Series B 58/5 (2003), 294; Catherine Theodosius, Emotional Labour in Health Care: The Unmanaged Heart of Nursing (London: Routledge, 2008), 5, 34, 41.
xxvi Sandra Bunkers, ‘The Lived Experience of Feeling Cared for: A Human Becoming Perspective’, Nursing Science Quarterly 17/1 (2004), 68-69; Patricia Benner, ‘Relational Ethics of Comfort, Touch, and Solace—Endangered Arts?’, American Journal of Critical Care 13/4 (2004), 349; Laura Funk, Sheryl Peters, and Kerstin Stieber Roger, ‘The Emotional Labor of Personal Grief in Palliative Care: Balancing Caring and Professional Identities’, Qualitative Health Research 27/14 (2017), 2218; Karen Iseminger, Francesca Levitt, and Lisa Kirk, ‘Healing During Existential Moments: The “Art” of Nursing Presence’, Nursing Clinics of North America, 44/4 (2009), 448; Kathleen Wilkin and Eamonn Slevin, ‘The Meaning of Caring to Nurses: An Investigation into the Nature of Caring Work in an Intensive Care Unit’, Journal of Clinical Nursing 13/1 (2004), 54.
xxvii Havi Carel, ‘A Reply to “Towards an Understanding of Nursing as a Response to Human Vulnerability” by Derek Sellman: Vulnerability and Illness’, Nursing Philosophy 10/3 (2009), 218.
xxviii John Ballatt, ‘Healthcare Culture and Intelligent Kindness in Practice’ in Compassion in Nursing: Theory, Evidence and Practice, ed. by Alistair Hewison and Yvonne Sawbridge (London: Palgrave, 2016), 92-105; Steven Ersser, ‘A Search for the Therapeutic Dimensions of Nurse-Patient Interaction’ in Nursing as Therapy, ed. by Richard McMahon and Alan Pearson (London: Chapman and Hall, 1991), 43-84; Martin Seager, ‘Who Cares for the Carers? Keeping Compassion Alive in Care Systems, Cultures and Environments: A Psychologically Minded Approach’ in Providing Compassionate Health Care: Challenges in Policy and Practice, ed. by Sue Shea, Robin Wynyard, and Christos Lionis (London: Routledge, 2014), 40-53.
xxix Katherine Froggatt, ‘The Place of Metaphor and Language in Exploring Nurses’ Emotional Work’, Journal of Advanced Nursing 28/2 (1998), 332-38; Funk, Peters, and Roger, ‘The Emotional Labor of Personal Grief in Palliative Care’; Susan McClement, Suzanne Wowchuk, and Kathleen Klaasen, ‘“Caring as If It Were My Family”: Health Care Aides’ Perspectives about Expert Care of the Dying Resident in a Personal Care Home’, Palliative & Supportive Care 7/4 (2009), 449-57; Moss et al., ‘The Metaphor of “Family” in Staff Communication About Dying and Death’.
xxx Andrew Ormsby, Ann Harrington, and Sally Borbasi, ‘“You Never Come Back the Same”: The Challenge of Spiritual Care in a Deployed Military Nursing Context’, Journal of Clinical Nursing 26/9–10 (2017), 1351, 1356.
xxxi Anna Castaldo, Maura Lusignani, Marzia Papini, Stefano Eleuteri, and Maria Matarese, ‘Nurses’ experiences of accompanying patients dying during the COVID-19 pandemic: A qualitative descriptive study’, Journal of Advanced Nursing 78/8 (2022), 2507-21; Jennifer Currin-McCulloch, Brooke Chapman, Colleen Carson, Kathleen Fundalinski, Magan Hays, Peggy Budai, and Shivani Kaushik, ‘Hearts above Water: Palliative Care during a Pandemic’, Social Work in Health Care 60/1 (2021), 93-105; Laura Green, Fiona Murphy, and Alice Davies, ‘“Into the Fire”: A Focus Group Study of Redeployed Staff during the COVID-19 Pandemic’, International Journal of Palliative Nursing 29/6 (2023), 274-80; Jacqueline Johnstone and Debbie Duncan, ‘Coronavirus: The 7th C Affecting the 6Cs. A Focus on Compassion, Care and Touch’, British Journal of Nursing 30/15 (2021), 928-33; Lucy Mitchinson, Anna Dowrick, Caroline Buck, Katarina Hoernke, Sam Martin, Samantha Vanderslott, Hannah Robinson, et al., ‘Missing the Human Connection: A Rapid Appraisal of Healthcare Workers’ Perceptions and Experiences of Providing Palliative Care during the COVID-19 Pandemic’, Palliative Medicine 35/5 (2021), 852-61; Michael Rabow, Chao-Hui Huang, Gloria White-Hammond, and Rodney Tucker, ‘Witnesses and Victims Both: Healthcare Workers and Grief in the Time of COVID-19’, Journal of Pain and Symptom Management 62/3 (2021), 647-56.
xxxii Ersser, ‘A Search for the Therapeutic Dimensions of Nurse-Patient Interaction’, 50-51.
xxxiii Katherine Roberts, Brian McAnany, and Martha Romney, ‘Nurses on the Front Line in the Coronavirus Pandemic and World War II: Parallels in Courage and Empathy’, (Unpublished study, Main Line Health: Lankenau Medical Center, 2021).
xxxiv Joyce Ffoulkes Parry, Joyce’s War: The Second World War Journal of a Queen Alexandra Nurse, ed. by Rhiannon Evans (Stroud: The History Press, 2015); Nell Jarrett, Diary. By the kind permission of Nell Jarrett’s family. Personal Collection of Jane Brooks; Vera Jones, A Time to Remember: A Record of Nursing Experiences, Impressions, and Travels during World War II Contained in Letters Sent Home from the East(London: Athena Press, 2005); Helen Luker, ‘Private Papers of Miss E.H.A. Luker’, Imperial War Museum, Documents.1274; Agnes Kathleen Dunbar Morgan, ‘Private Papers of Miss A.K.D. Morgan: Still with the Lamp’, Imperial War Museum, Documents.16686; Mary Morris, A Very Private Diary: A Nurse in Wartime, ed. by Carol Acton (London: Weidenfeld & Nicolson, 2014); Betty Murgatroyd, ‘Private Papers of Miss B. Murgatroyd’, Imperial War Museum, Documents.19944.
xxxv Elizabeth Baer, ‘Ambivalence, Anger, and Silence: The Civil War Diary of Lucy Buck’, in Inscribing the Daily: Critical Essays on Women’s Diaries, ed. by Suzanne Bunkers and Cynthia Anne Huff (Amherst: University of Massachusetts Press, 1996), 210; Michael Roper, ‘Splitting in Unsent Letters: Writing as a Social Practice and a Psychological Activity’, Social History 26/3 (2001), 319, 337-338; Penny Summerfield, ‘Culture and Composure: Creating Narratives of the Gendered Self in Oral History Interviews’, Cultural and Social History 1/1 (2004), 68.
xxxvi Roberts, McAnany, and Romney, ‘Nurses on the Front Line’, Respondent 11998695427.
xxxvii Ibid., Respondent 11996723842.
xxxviii Ibid., Respondent 11977934385.
xxxix Morgan, 52.
xl Brooks, Negotiating Nursing, 65.
xli Morgan, 52.
xlii Jarrett, 8 November 1942, 118.
xliii Karin Hugelius, Nahoko Harada, and Miki Marutani, ‘Consequences of Visiting Restrictions during the COVID‐19 Pandemic: An Integrative Review’, International Journal of Nursing Studies 121 (2021), 9.
xliv C. Abad, A. Fearday, and N. Safdar, ‘Adverse Effects of Isolation in Hospitalised Patients: A Systematic Review’, Journal of Hospital Infection 76/2 (2010), 97; Hugelius, Harada, and Marutani, ‘Consequences of Visiting Restrictions during the COVID‐19 Pandemic’, 1.
xlv Roberts, McAnany, and Romney, ‘Nurses on the Front Line’, Respondent 11997363897.
xlvi Ibid., Respondent 12021249606.
xlvii Morris, A Very Private Diary, 223.
xlviii Benner, ‘Relational Ethics of Comfort, Touch, and Solace’, 346.
xlix Ibid., Respondent 12018197406.
l Ibid., Respondent 11996732542.
li Ibid., Respondent 12026626107.
lii Ibid., Respondent 12021029965.
liii Ibid., Respondent 11977934385.
liv Newsletter courtesy of Joanna Dixon, ‘Wads Words: Connecting with Barbara Wadsworth’, 27 April 2020.
lv Morgan, 146.
lvi Ffoulkes Parry, Joyce’s War, 64.
lvii Morris, A Very Private Diary, 123.
lviii Bunkers, ‘The Lived Experience of Feeling Cared for’, 64; Deebs Canning, John Rosenberg, and Patsy Yates, ‘Therapeutic Relationships in Specialist Palliative Care Nursing Practice’, International Journal of Palliative Nursing 13/5 (2007), 223; Iseminger et al., ‘Healing During Existential Moments’, 448, 451; Wilkin and Slevin, ‘The Meaning of Caring to Nurses’, 54.
lix Belinda Dewar, Richard Mackay, Stephen Smith, Simon Pullin, and Ria Tocher, ‘Use of Emotional Touchpoints as a Method of Tapping into the Experience of Receiving Compassionate Care in a Hospital Setting’, Journal of Research in Nursing 15/1 (2010), 36-37; Canning, Rosenberg, and Yates, ‘Therapeutic Relationships in Specialist Palliative Care Nursing Practice’, 223.
lx Carden-Coyne, The Politics of Wounds, 10, 214, 338.
lxi Hallett, ‘Emotional Containment’, 256.
lxii Roberts, McAnany, and Romney, ‘Nurses on the Front Line’, Respondent 12000290085.
lxiii Ibid., Respondent 11996730777, respondent 11977934385.
lxiv Ibid., Respondent 11977934385.
lxv Lupton, ‘“Your Life in Their Hands”’, 168.
lxvi Roberts, McAnany, and Romney, ‘Nurses on the Front Line’, Respondent 12017015891, respondent 11996606112.
lxvii Morgan, 52.
lxviii Morgan, 50.
lxix Morris, A Very Private Diary, 162.
lxx Morgan, 143.
lxxi Jones, A Time to Remember, 233.
lxxii Ffoulkes Parry, Joyce’s War, 144.
lxxiii Morgan, 231.
lxxiv Lupton, ‘“Your Life in Their Hands”’, 168.
lxxv Jones, A Time to Remember, 297.
lxxvi Ibid., 315.
lxxvii Luker, 18 February 1940.
lxxviii Ibid., 24 February 1940.
lxxix Morgan, 35.
lxxx Roberts, McAnany, and Romney, ‘Nurses on the Front Line’, Respondent 11996723842.
lxxxi Ibid., Respondent 11973549481, respondent 11973511975.
lxxxii Ibid., Respondent 11997363897.
lxxxiii Jones, A Time to Remember, 291.
lxxxiv Ibid., 315.
lxxxv Roberts, McAnany, and Romney, ‘Nurses on the Front Line’, Respondent 12017818068.
lxxxvi Ibid., Respondent 11996717994.
lxxxvii Brooks, Negotiating Nursing, 45.
lxxxviii Roberts, McAnany, and Romney, ‘Nurses on the Front Line’, Respondent 11997363897.
lxxxix Ibid., Respondent 11998695427.